The (CAF): An Approach to Strengthen Community Ownership to Improve the Quality of Care in TB Services
The (CAF): An Approach to Strengthen Community Ownership to Improve the Quality of Care in TB Services
Introduction and Rationale
The Community Accountability Framework (CAF) is an approach where the TB Champions act as a bridge between the community and the healthcare system to draw attention of the health care systems to community-based issues concerning health care. In doing so, communities work in coordination with healthcare providers through a consultative process to improve outcomes of TB treatment and care. Thus, it attempts to bring in the persons with TB (PwTB) their caregivers and the TB champions as ALLIES to the TB program. CAF as an approach recognizes the rights and responsibilities of both PwTB and healthcare systems. Hence, the role of TB Champions is pivotal, as they play the role of community advocates in a consultative process with the healthcare providers to improve the quality of TB care services for their communities.
Objectives
To improve the environment for TB elimination by promoting community action for accountability.
Overall approach and Key Strategies
A comprehensive tool, specially designed for the purpose, has defined parameters of ‘Timeliness’, ‘Accessibility’, ‘Quality of information’, and the existence of stigma associated with TB at different levels. These parameters that are part of the CAF assessment are in line with the priority quality indicators under the National TB Elimination Programme (NTEP). This CAF tool is used with the PwTB to assess the gaps. Based on the identification of gaps, TB Champions themselves generate their Block Action Plans (BAP) for addressing those prioritized gaps. TB Champions implement their BAP based on locally available resources and local solutions, thus making the solutions community-centred and community-led. This in turn ensures that the community can hold health systems accountable for TB care services. Thus, this is a cyclical approach to redress the identified gaps in each cycle to bring quality to the TB care program.
Implementation
These CAF processes are being implemented in three districts of Odisha, namely, Angul, Bhubaneshwar, and Mayurbhanj, keeping high burden TUs a priority. These include eight TB units (TUs) in Angul, a district of the industrial belt; three TUs in Bhubaneswar, an urban belt, and 17 TUs in Mayurbhanj, a district in the tribal belt. The implementation of CAF was initiated in April 2021 and is continuing. Through this process, the following are the major activities that are undertaken: local level advocacy with Health Care Providers (HCP), Panchayati Raj Institution members, and other community-based stakeholders; community level awareness programs; addressing TB relating stigma; supporting family visits, and contact tracing in coordination with HCPs. This project (ALLIES) is being implemented by REACH with support from the United States Agency for International Development (USAID).
Outcomes
There have been significant improvements over this period with the active support of the TB care program in the areas of Ni-kshay Poshan Yojana, treatment adherence, psychosocial support, family visits, counselling, and so on. The following graphs highlight the trends.
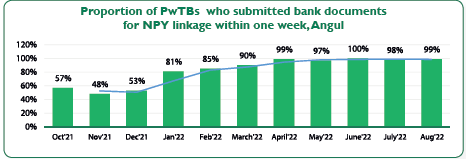
Graph-01: Proportion of PwTBs who submitted bank documents for NPY linkage within one week, Angul
Graph-01 shows the trend of bank seeding within a week of treatment registration. The graph shows how coordination and consultation at the field level contributed to the improvement of this indicator over a period of time. During the CAF implementation process, hand-holding support towards bank linkages under NPY and coordination at the community level is evident in the positive trends of this indicator.
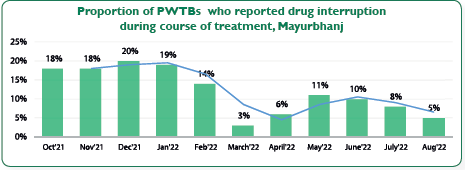
Graph-02: Proportion of PWTBs who reported drug interruption during course of treatment, Mayurbhanj
Graph-02 shows the trends in responses of PwTB from the TUs of Mayurbhanj who were assessed under CAF on their drug interruption over the months from October 2021. The dip in data on drug interruption depicts a significant impact on treatment adherence due to the regular coordination and consultation between the treatment supporters, PwTB, and health staff.

Graph-03: Proportion of PwTB initiated on treatment within 3 days of diagnosis, Mayurbhanj
Graph-03 shows the trends in the timeliness of the treatment initiation. The data covered here are of responses from persons with Drug sensitive TB (DSTB) in Mayurbhanj. There have been positive trends over this period in the treatment initiation within an ideal time frame, i.e. 3 days of diagnosis. With the active involvement of TB Champions in coordination with the health staff in Mayurbhanj, this margin of delay in treatment initiation has been addressed, and by end of August 2022, 99% of PwTB reported that they had initiated their treatment not later than 3 days from the time of their diagnosis.
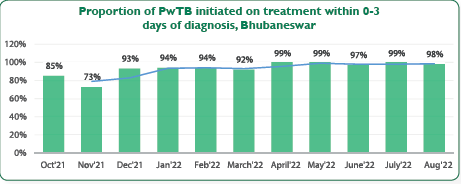
Graph- 04: Proportion of PwTB initiated on treatment within 0-3 days of diagnosis, Bhubaneswar
Graph-04 shows the trends of timeliness in initiating the treatment. The data covered here is of responses from people with DSTB who are currently on treatment. It shows the positive trend over these periods in the treatment initiation in an ideal time frame, i.e. 3 days of diagnosis, through regular consultation by the TB Champions in Bhubaneshwar with the Senior TB Supervisors and TB Health Visitors. It has addressed this margin of delay in treatment initiation, and by end of August 2022, 98% of PwTB reported that they had initiated their treatment within 3 days of their diagnosis and not later than that.
Key Recommendations
- Handholding support and coordination between HCPs and TB Champions can strengthen the TB elimination programme.
- Utilizing the expertise of TB Champions as community mobilizers and advocates can strengthen the TB response.
- TB Forum Meeting are opportunities for TB Champions to share their best practices and enable a consultative process to help improve the quality of care and services in TB.
- Cross-learning visits between districts are an opportunity to highlight the innovations of district programs for a positive impact on TB elimination in the state.
Potential for Replication and Scale-Up
CAF is a participatory approach that can bring accountability in TB care services. Since presently it is being implemented in three districts in Odisha, and there are TB Champions in every district, this could be an ideal approach to replicate and roll out across the districts/state.
Source : TBC India
Last Modified : 5/30/2023
A case study of the initiative of an Anganwadi wor...
This topic provides information about Promotion of...
This topic provides information about Integration ...
This topic provides information about PRI sensitiz...